Friday, November 19, 2021
Covid Update: VFR
My Covid updates have stalled while I've been waiting for any sort of all-cause mortality data to come out. And waiting. And waiting. The stark absence of such data is itself very revealing[2].
But it turns out some slipped out late October, brought to my attention yesterday by Alex Berenson.
I thought it was worth a more thorough analysis, so here it is:
TLDR: If this data holds up, the vaccines are killing more people than they are saving. Curious? Read on.
The basic setup is this:
The study in question looks at Scandinavian-thorough data for some four million Swedes, and shows that vaccine efficacy starts out good but wanes over time, thus serving the current narrative push for boosters. It's a big study and, although not yet published, appears to be fairly well done. I expect it answers the questions it asks reasonably well.
But, of course, they're only allowed to ask the wrong questions, because that's how sciencism works these days.
So let's ask the right ones. Bear with me as I zip through this -- the reasons for it all will become evident below.
On figure one (page 32 of the pdf at this time) they say:
"From this cohort, 4,034,787 individuals were identified that had two shots of vaccine no later than August 5."
From which:
"Excluded: 3,939 Died within 14 days of [date of second dose]."
Now, Alex does some back of the envelope calculations for what this number ought to be, but rightly observes that timing matters since, e.g., if these were all in the winter, the expected death rates would be higher (over 4k per 2 weeks). And he also relies on extrapolated data from prior years which is hazardous when death rates and numbers are steadily changing year to year as evidenced in my prior covid update.
So, let's not make any guesses. Let's actually calculate how many people should have died in that window. Here's how we do it:
First, we take the number of Swedes fully vaccinated, by date and age group:
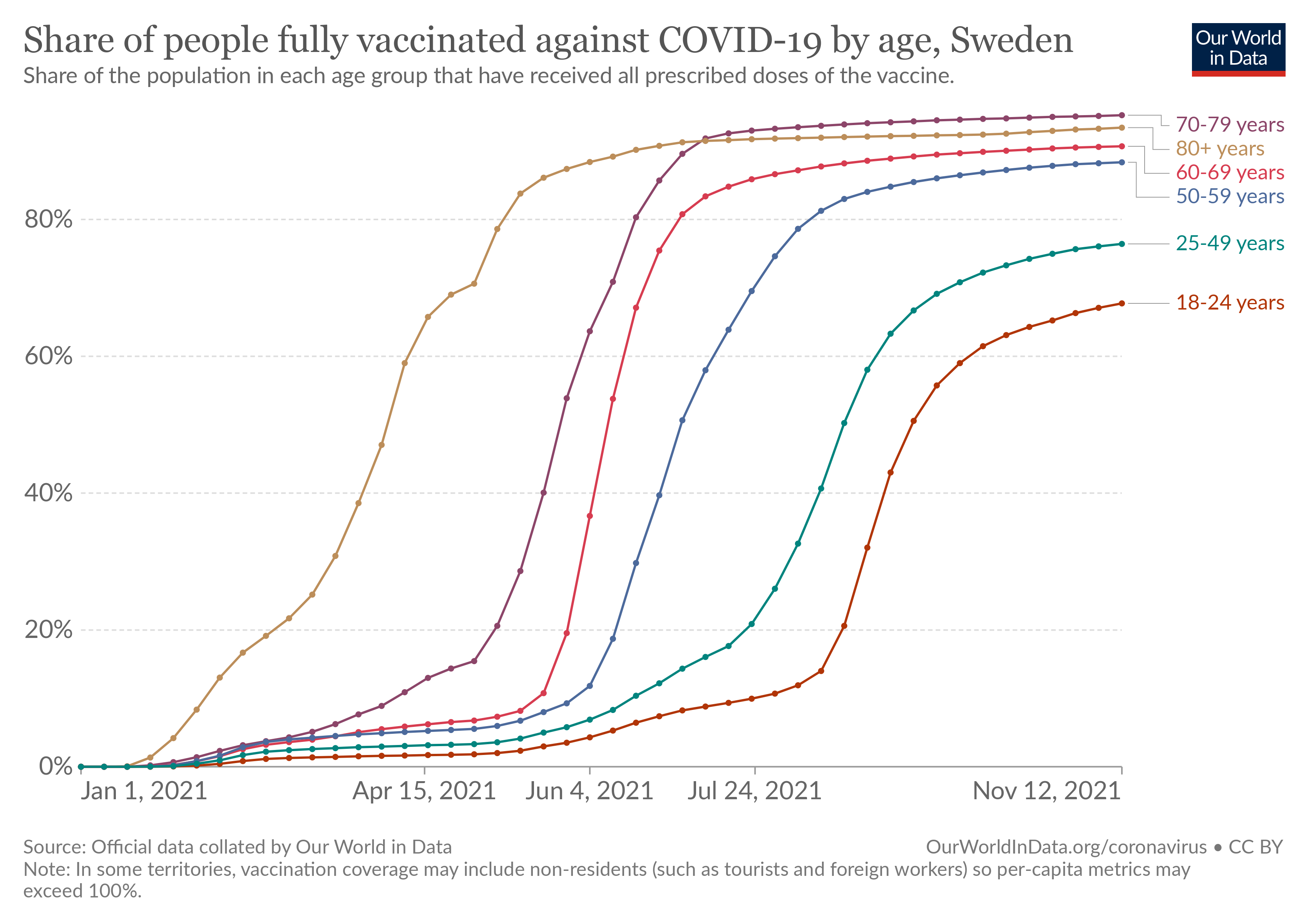
This results in about 4.5 million people who had their second dose during the time window covered by the study, with an average age of 59.1 and an average second-dose date of 2021-06-02. The larger study group in the paper, selected from their ~4 million cohort, had an average age of 59.4 and an average second-dose date of 2021-05-19. So, our sample (the full sample of all second-doses in Sweden) is very representative of the study sample.
Next, we combine that with the actual number of deaths in Sweden during the study window:
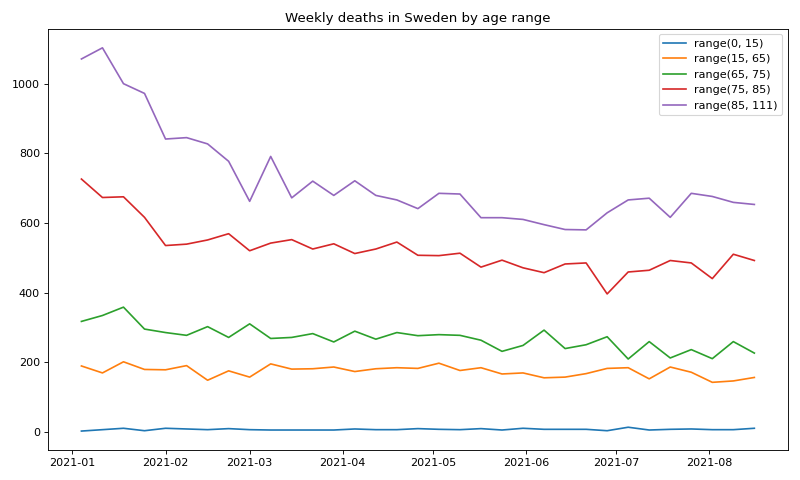
This is not us extrapolating some expected number of deaths from past years--this is the actual number of all-cause deaths in Sweden for each week of the study, by age group. Also, we can (and I did) further extrapolate the distribution of those deaths within each age group using historical death distributions, which does not change the number of deaths at all but lets us (to a reasonably good approximation) distribute them more accurately among the mis-aligned vaccination age groups.
After adjusting for the 4/4.5 million ratio (since they did not use quite all of the fully vaxxed people like we are), the net result is, to a very good approximation, the number of deaths we should have seen in the study in the two weeks following the second doses, assuming there is no correlation with the vaccine and all-cause mortality at all. Indeed, if the vaccines lower all-cause mortality in that window, as the CDC recently claimed, then the expected number should be higher than the actual number (3,939).
Running the calcuations, we get an expected 2,640 deaths.
That means there were 1,300 more deaths in the two weeks following the second dose of the vaccine than there should be. I say "should" as opposed to merely "we might expect" because this is based on actual numbers of deaths (can I emphasize that too many times?) and actual second-dose dates by fairly narrow age bands. The most significant assumption in this particular calculation is that the vaccinated population is not a priori significantly more at risk of death than average. If you look at the study's demographics, the vaxxed group does in fact appear to be a bit less healthy than their age-matched unvaxxed counterparts, so this is a real confounder, however the impact is not likely to be large here[1] -- even if they represented 100% of all Sweden's fatalities (an absurd extreme) there is still a significant deficit as Alex observed in his initial back-of-the-envelope upper limit. Furthermore, this is just for the second dose, and only for the immediately following two weeks, which means we are under-counting by however many causal deaths happened after the first dose or after two weeks (not unlikely for cardio issues). Let's call that a wash even though I suspect the true number is even worse.
Now, we don't know anything about how those excess deaths were distributed (over time or age), but we do know how many doses likely caused them, so can calculate, for roughly the currently fully-vaccinated population of Sweden as a whole (since that's roughly our study cohort):
VFR (vaccine fatality rate) = 0.03%
Or about 1 extra death per 3,100 second doses, just in the first two weeks after the dose.
In the original Pfizer trial, this would equate to about 6 excess deaths (of 19k vaxxed). But Pfizer used an atypically healthy cohort with an average age of only 50.4, so we should expect less. The actual difference was 5 (not 1 like their public study release claimed), and that's assuming they didn't bury more. (Yes, that's right -- all-cause mortality in the Pfizer RCT was 24% higher in the vaxxed arm. Nothing to see here, move along.)
If we assume Americans are biologically similar to Swedes, then, based on the number of fully vaccinated, that translates to about 63,000 Americans killed so far by the second dose alone. This is on the same order as a number of other estimates (from VAERS, etc), which typically have put the figure at about 120,000 conservatively for all doses and latencies.
So, yeah.
But wait, there's more...
The cited study also happens to show that vaccine efficacy for symptomatic infection goes negative by about 9 months--something we are also seeing in the UK data.
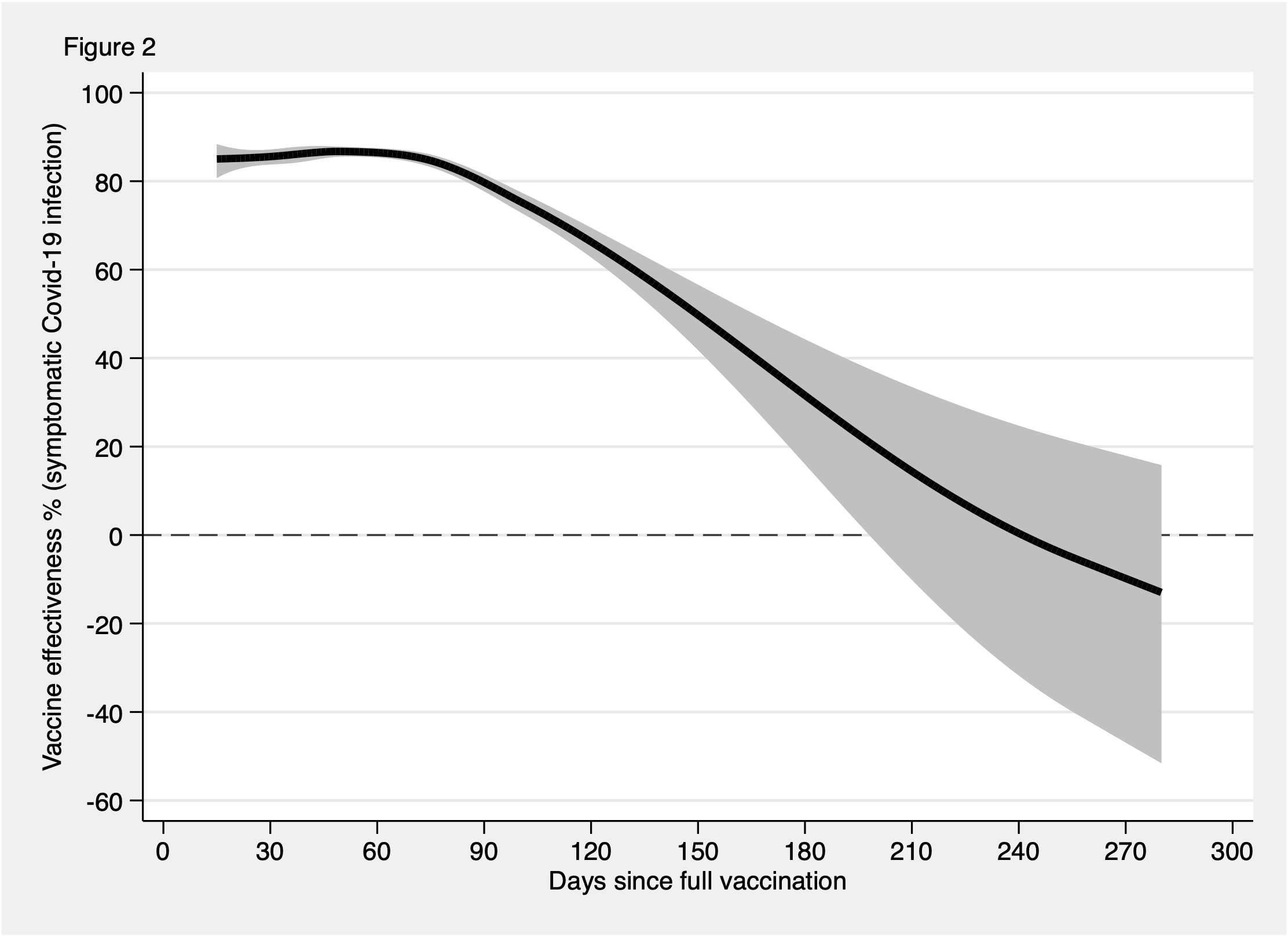
But the efficacy against hospitalization and death remains positive throughout, which is the high point of these vaccines: Even if they're doing a crap job of preventing transmission, they protect you, at least. Right?
Right?
Turns out, NOPE.
What they appear to do is kill you if you're weak or especially sensitive to the spike protein, so that Covid can't kill you later. Okay, that's wild extrapolation, but amiwrong?
Take the following with a grain of salt because it depends on how much covid is going around at the time, but:
If we assume about 25% of hospitalizations lead to death (higher numbers make the vax look better so I'm conservatively erring on the high side), then even by six months after the vax, when its effectiveness had significantly waned and so the bulk of its benefit was over, fewer people in the above study had been spared death-by-covid than were killed in the first two weeks by the vaccine itself. As a ballpark, for every 5,000 second doses they killed one person on net. That would be equivalent to about 40,000 people needlessly dead in the US to date (depending on how similar the covid waves were).
Bottom line, the vaccine efficacy for all-cause death appears to be negative across the board--you're less likely to die if you don't take it. (And there's every reason to believe the boosters will be significantly worse. Early signs support this.)
So, yeah.
How'bout them mandates?
[1] Update 2021-11-20: If we shuffle the deaths between groups so that our vaxxed population are twice as likely as the unvaxxed to die a priori, the excess deaths drop from 1300 to 1170--only about 10% and with negligible impact on the VFR. So this is unlikely a substantial bias.
[2] Update 2021-11-20: Re. the recent all cause mortality data from the UK, see this overview. (Note in particular the very final graph.) Update 12/3: See also Possible systematic miscategorisation of vaccine status raises concerns about claims of Covid-19 vaccination effectiveness And The importance of the delay between infection and death in official statistics
[3] Update 2021-11-22: Just found this study (October preprint) which tries to estimate the VFR from correlations of excess mortality with vax uptake across various countries, and comes up with 0.04%, which is very close to my 0.03%: COVID vaccination and age-stratified all-cause mortality risk
[4] Update 2022-07-14: The Rollout of COVID-19 Booster Vaccines is Associated With Rising Excess Mortality in New Zealand estimates 0.016% VFR in New Zealand from the boosters.