Thursday, October 06, 2005
Tee Minus-Five
I now have four opinions in favor of surgery (including one rational-variety chiropractor who normally avoids surgery at all costs) and zero against. All of them seem to think I'm a sneeze away from total paralysis. Surgery is scheduled for Tuesday. If I croak, somebody please post notice here.
Far and away the most observant and specific analysis of the four came from an old acquaintance/friend-of-friend who happens to be an expert in just this sort of thing:
[...] Based on these MRI findings in conjunction with your x-ray findings, I think you will need surgery. Here are my reasons:X-ray findings: The fact that your vertebra shifts that much between laying flat and standing up is very worrisome. If the added vertical load caused by the weight of your head upon your spine merely by going from laying down to standing up is enough to cause that degree of change, it means that one of your C5-6 facet joint is significantly weakened and that relatively minor trauma could cause it to shift more. As I'm sure you noticed, there isn't any significant malalignment when you're laying flat.
MRI findings: Because your MRI was obtained when you were laying flat, there is no malalignment of the facet joints at the time the images were acquired. But there are a number of extremely disturbing signs that are present. I've gone ahead and attached set of annotated JPEG's so you can see what I'm talking about. Although these are magnified, the series and image numbers are included in the upper left corner, so you can correlate them to the images on your CD.
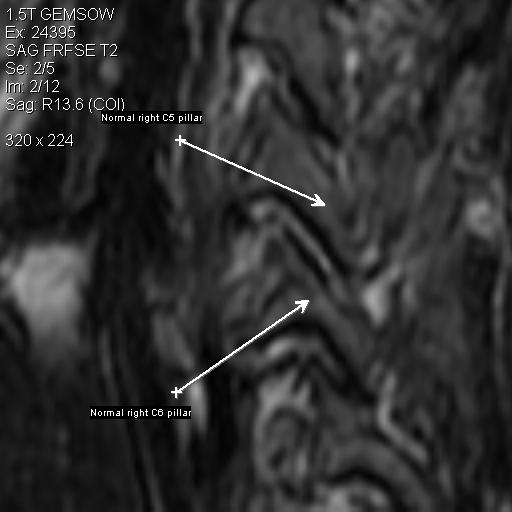
This shows the normal alignment of the C5-C6 facet joint on the right side. I've included this so you have a normal baseline for visual reference.
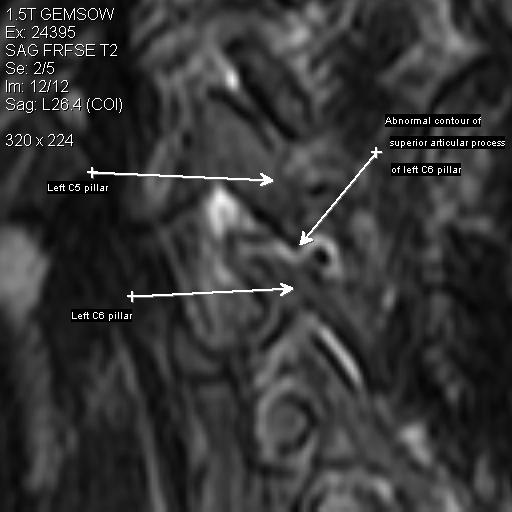
This shows a subtle irregularity to the contour of the superior surface (aka "superior articular process") of the left C6 pillar at the left C5-C6 facet joint. So that made me suspicious.
The arrow is pointing to a tear of the "ligamentum flavum", one of the primary stabilizing ligaments of the posterior margin of the bony spinal canal. You can see that there is an interruption of the normal black vertical line posterior to the (grey) spinal cord and the (white) spinal fluid.

This shows the post-traumatic disc bulge at C5-6. The thin vertical black line that forms the posterior border of the disc is a combination of the disc capsule (aka "annulus") and a key ligament known as the "posterior longitudinal ligament" (PLL). The PLL is a key stabilizer of the vertebral bodies, located at the anterior margin of the bony spinal canal.
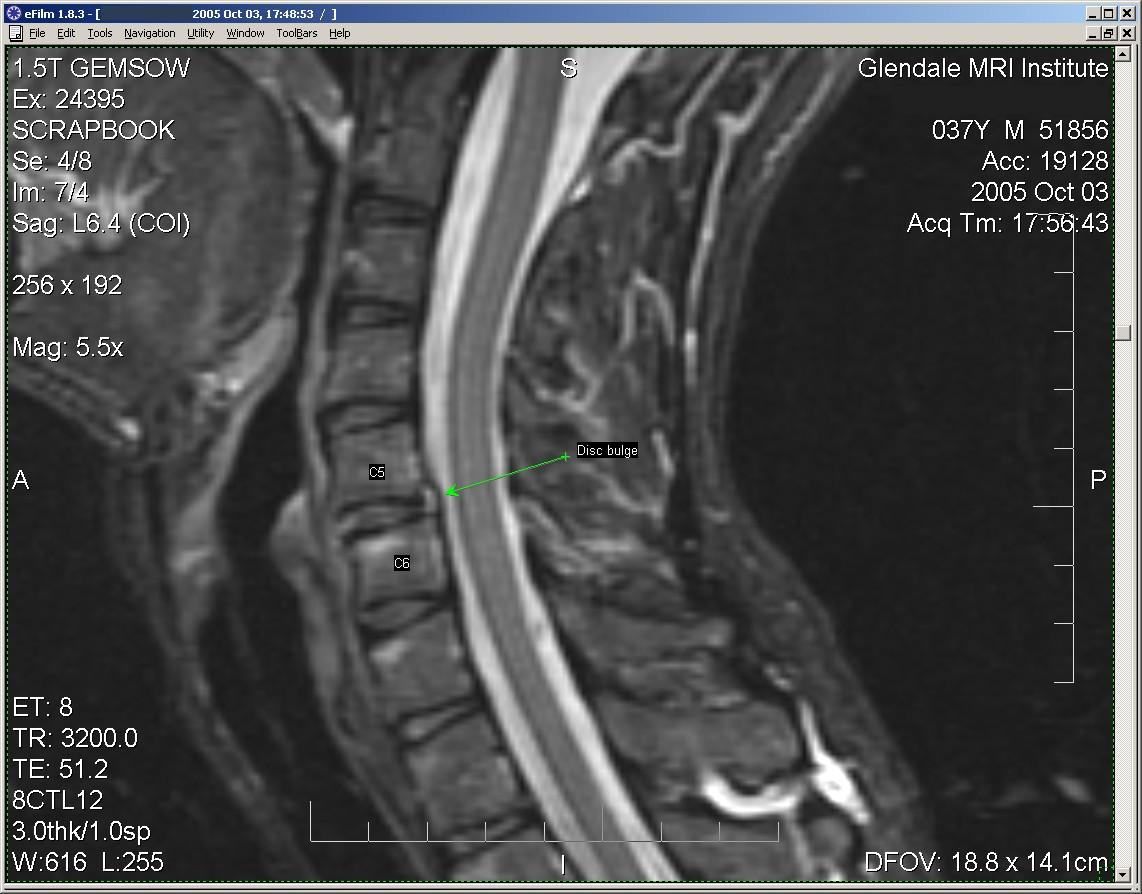
Here is a partial tear of that posterior longitudinal ligament. It is this tear that allows your C5 vertebral body to shift relative to C6 when subjected to stress.

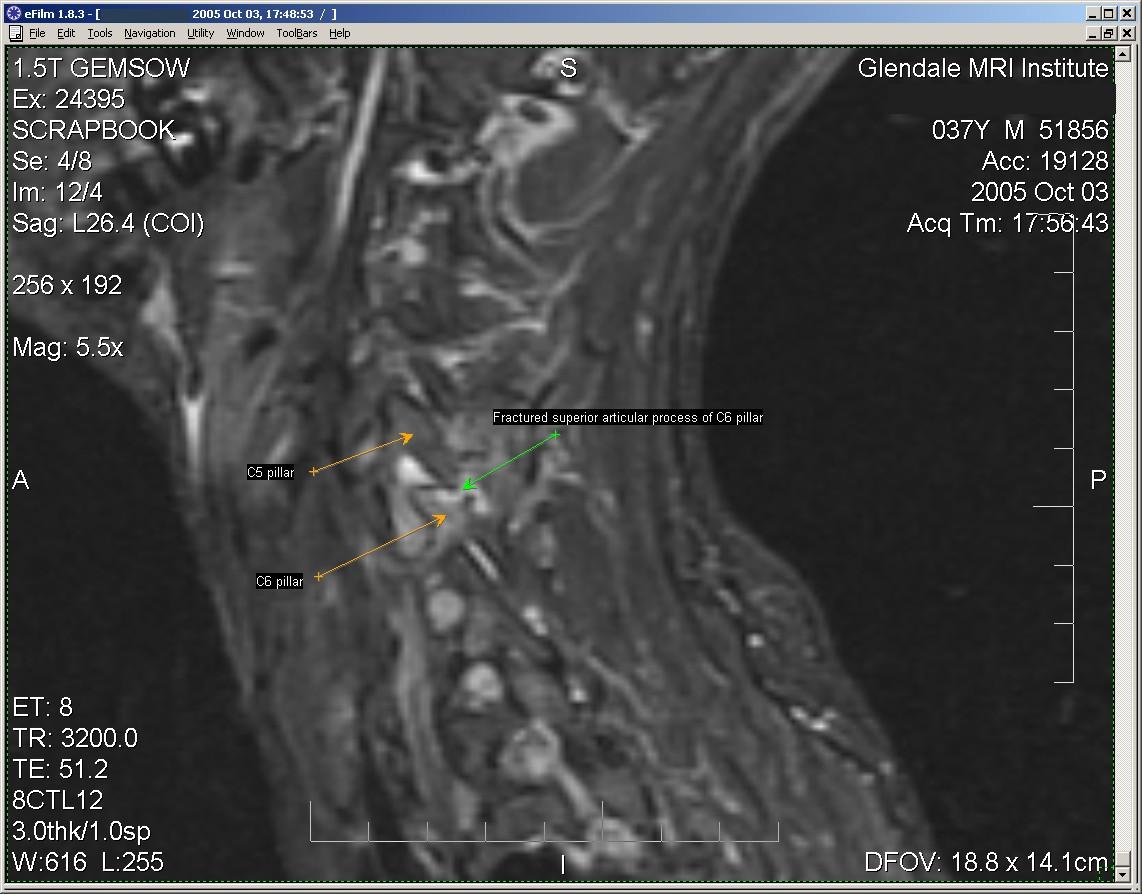
This is another view of the abnormal left-sided C5-C6 facet joint. The arrow points to a fracture of the superior articular process of C6 (which was the area that looked funny on [image 2, above]). This particular MRI pulse sequence has lower spatial resolution, but increased sensitivity for subtle fractures. My guess is that the fracture at this site allows the left sided C5 pillar to move with respect to the C6 pillar when you are subjected to a vertical load.
Hence, given the combination of a posterior longitudinal ligament tear, a ligamentum flavum tear, and a C6 pillar fracture, there are enough disrupted elements that you are at a very high risk of catastrophic spinal injury (i.e., permanent paralysis) with relatively minor additional trauma.
Some spine surgeons speak in terms of the 3 vertical stabilizing "columns" of the spine. You've disrupted elements of the middle and posterior columns. (An isolated single column injury can often be treated without surgery, but 2 and 3 column injuries usually do require surgery.)
[...]
I hope you find this information helpful, Simon. Please let me know how things go with you.
In the meantime, I urge you to be extremely careful in your daily activities. If you're not in some kind of protective neck collar, you should strongly think about getting one. You also should not go bicycling, etc., until this situation is adequately addressed.
Good luck!
---------------------------------------
Paul S. Hsieh, MD